

In Brief: A practical roadmap for where objective cognitive measurement fits in a private psychiatry practice, and how it streamlined my clinical workflow without compromising care. Written for any psychiatrist who, like me, once hesitated to change a routine that already works.
When I moved to California from Chicago several decades ago, I found that the preconceived notions I held about California culture were actually true: it really is sunny and 75 degrees every single day, you really can ski and surf on the same day, and movie stars really are just like us (as evidenced by the frequent star sightings I experience at the grocery store and beyond). The most pervasive of these notions was that a person (me) should be practicing yoga and meditating all the time. I was bombarded with invitations to join yoga studios, entreaties from friends boasting tales of baby goats scaling the sculpted backs of serene yogis, and reminders from my husband (a fellow physician and native Californian) of the health benefits I was missing by declining his daily sunrise flow and nightly meditation hour.
I had my own reasons for resisting, but suffice it to say I avoided the practice of both yoga and meditation for over two decades. I truly had no idea what I was missing, and I truly did not care. Then COVID and lockdown hit and something inside me clicked. I accepted that it was time to explore what I had resisted for so long. So I went all-in, and I loved it. I loved it so much that I not only engaged in daily practice but became a certified yoga teacher and mindfulness and meditation instructor – both of which required a basic understanding of Buddhism and its tenets. The benefit to my life, and to my physical and emotional health, cannot be overstated. It truly changed my life.
As I think about why digital tools are not yet widely used in psychiatry and behavioral health despite their proven usefulness, and why I resisted these tools in my own practice for so long, I am reminded of my resistance to yoga and meditation, and of the benefits I have experienced since letting go of it. There is a concept in Buddhism that describes habits, both mental and behavioral, as grooves worn into our minds through repeated thought and action. Because I am an artist as well as a physician, I like to think of this in tactile terms, imagining I'm running my finger across the deeply engraved copper plate of my mind, waiting to be filled with the ink of my daily life and work.
Over 20 years ago, as a PGY-1 psychiatry resident, I was taught to conduct the traditional psychiatric assessment. I practiced it day after day until every question was imprinted on the copper plate of my mind. The assessment, and the workflow around it, became second nature. It worked, and it worked well.
These routines shaped my approach to patient care and gave my days a sense of comfort and predictability. So when new digital tools arrived, I was hesitant, preferring the familiar methods I had refined over the years. Why change a good thing?
It's easy to feel overwhelmed at the thought of changing a workflow that, well, works. But yoga teaches that habits can keep us from growing, and that through observation and self-reflection we can reshape them. In other words: change can be good. And rethinking the traditional psychiatric assessment can benefit not only our patients but ourselves. So I took a leap and learned everything I could about the technologies I had been resisting. What I learned transformed my practice.
Adopting digital assessment tools in the outpatient practices I direct helped me streamline evaluations, reduce the note-taking and administrative burden, and support high-volume psychiatric care without compromising care quality. These demonstrable benefits also made it easier for the multi-provider groups I manage to embrace them.
The Workflow I’d Been Using Wasn’t Designed to Measure
I rely on the traditional psychiatric assessment, gathering information through observation and self-reported symptoms that inform my treatment decisions. The face-to-face interview remains integral to my practice. Nonetheless, it often prompts me to consider whether crucial information has been overlooked, and what it would take to address those gaps.
Further, the traditional workflow psychiatrists use today has been shaped by several challenging realities. These include strict time constraints, overwhelming caseloads, and reimbursement systems so complex that change can feel nearly impossible, even when we identify an area that needs improvement, like cognitive assessment.
Cognition: The Hidden Infrastructure of Mental Health
Psychiatrists assess cognition through observation and patient self-report as part of the traditional initial evaluation but often lack the tools, time, and resources needed to formally measure cognitive deficits. Because the traditional approach relies heavily on symptom identification and diagnostic frameworks, it remains limited in its ability to catch subtle changes in cognition.
Cognition relies on interconnected neural networks that support our domains of functioning. Cognitive functions like orientation, learning, problem-solving, reasoning, memory, and judgment depend on these domains working properly, which psychiatric conditions often disrupt.
Because these disruptions are difficult to detect early, we can miss subtle shifts in cognition, shifts that are especially important to identify because they are core characteristics of the psychiatric disorders we treat.
Psychiatric disorders with notable cognitive deficits include:
- Major Depressive Disorder: Cognitive impairment like disordered attention, memory, and executive functioning. In severe cases, deficits can mimic dementia, with impairment persisting even in euthymic states.
- ADHD: Early cognitive symptoms like decreased attention, memory deficits, delayed comprehension, and difficulty shifting mental strategies are typically present before formal schooling, which makes them especially difficult to identify. Common ADHD symptoms like decreased sleep and emotional dysregulation also impair cognitive function.
- Schizophrenia: Cognitive deficits are a core feature and include problems with perception, attention, memory, and problem-solving, most commonly when disorganized and negative symptoms prevail. These deficits resist existing treatments and result in impaired functioning and markedly decreased quality of life.
- Autism Spectrum Disorder: Cognitive deficits can begin well before formal schooling and include impairment in executive function, memory, and attention; social cognitive deficits; language and communication delays; and difficulty integrating and processing sensory input.
- PTSD: Difficulties with memory and recall, trouble processing trauma, subjective "brain fog," and impaired attention are all cognitive deficits that may be subtle and difficult to identify in people who have experienced trauma.
Where Objective Data Actually Fits in the Clinical Flow
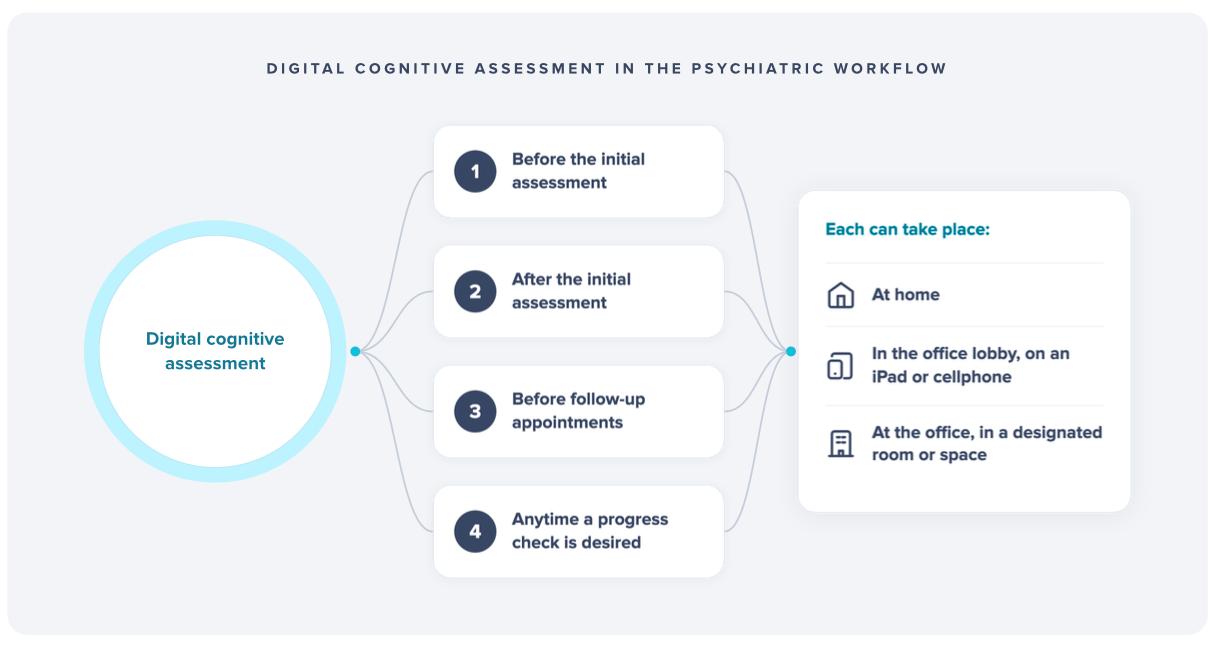
Patient assessment is a continuous process rather than a single event, an ongoing journey woven throughout the psychiatric workflow. Initial assessment, follow-up, medication management, and longitudinal monitoring are all distinct stages of care that rely on the clinical judgment and expertise of experienced clinicians, and each can be augmented with digital assessment tools.

In my practice, integrating digital tools has measurably improved the quality of patient care. With these tools, I can augment subjective clinical observations with more consistent, objective assessments at every stage of treatment.
The data I collect objectifies symptom severity and lets me reliably track progress and response to treatment over time. Comprehensive objective data informs treatment goals and helps me make care decisions aligned with the standard of care. It supports an evidence-based practice and helps ensure each patient's needs are met with precision.
Plus, this data creates a shared language between my patients and me. It improves the tone of our treatment conversations, builds reassurance into our decisions, and increases patient engagement. When patients see that my clinical decisions are backed by objective data, they feel more confident and involved in their care.
Intake and Initial Assessment: Building a Baseline That Holds
Psychiatric assessment begins with the traditional interview, where observation and patient self-report help identify symptoms, history, and risk factors. Often, this process feels less like a starting point and more like being dropped into the middle of a marathon, tasked with assessing how the first half of the race went without having watched it.
We are asked to gather large amounts of information in a short time from patients who are suffering, all while asking them to "start at the beginning." Whether or not we are their first contact with psychiatry, establishing a reference point for future care is essential. Digital cognitive assessments administered at this stage help frame baseline data, ensuring relevant factors are considered early in treatment.
This investment saves time by reducing redundant assessments and inconsistent documentation, especially in group practices like the ones I create, where patients see multiple providers. It spares us from piecing together fragmented information and keeps the workflow streamlined.
Follow-ups: Moving From “How Are You Feeling” to Evidence
Follow-up visits are essential for tracking treatment progress, adjusting goals, and addressing new patient needs. A large part of follow-up involves asking patients to report their symptoms, which depends on their ability to accurately recall and describe how they feel during brief appointments. Without objective measurement, these sessions offer limited, episodic snapshots of symptoms.
Seeking more depth and objectivity, I integrated digital cognitive assessment tools into my workflow, using them before, during, or after follow-up visits at a typical cadence of every 3 to 6 months. This shift gives me trend-based insight, letting me monitor objective change over time. It also helps my patients gain a clearer understanding of their progress.
Medication Management: When Data Reduces the Guesswork
Medication management is a crucial aspect of psychiatric care, but the subjective nature of psychiatric assessment often leaves me with some clinical uncertainty when choosing and adjusting medications. While certain drugs are expected to produce specific outcomes at specific doses, psychiatry lacks exact predictability, so I cannot always anticipate how a patient will respond to treatment.
Integrating Creyos into my outpatient workflow has added structure and objective data to my medical decision-making that symptom report alone cannot. For example, I saw a notable improvement in my ability to diagnose and manage ADHD in my adult patients.
A 21-year-old college student with ADHD was stable on stimulants and reported no issues 8 months into treatment. They said they were doing "great," and from their perspective, everything was status quo. But because I was monitoring their treatment progress with digital cognitive testing, I identified a troubling trend: their sustained attention scores had declined markedly from their initial baseline over the past several months. Their reaction time variability had also increased – another sign that their current medication regimen might not be working as effectively as it should. Upon further questioning, they admitted to staying up later than usual to study and steadily increasing their caffeine consumption, a fact they had not realized until they saw how much their spending had increased at Starbucks. This data guided my recommendation for a medication adjustment, which improved their academic performance while reducing both study time and caffeine intake.
Longitudinal Monitoring: What You Can Only See Over Time
Psychiatry is not a one-and-done specialty. Unlike a broken bone that can be placed in a cast and "cured" in 6 to 8 weeks, mental health is not static. Moods rise and fall, functioning fluctuates, and symptoms can appear or worsen unexpectedly.
Digital tools let me track these shifts over time, offering objective data alongside my traditional assessments and follow-ups. By combining both methods, I gain a clearer picture of my patient's symptoms and feel more confident evaluating their progress.
Subtle changes, such as gradual increases in symptom scores, may signal emerging issues even when symptoms remain mild. When symptoms are improving, plateauing, or worsening, objective data lets me see how that aligns with what I observe and what my patients report. That gives me a broader perspective on their symptom trajectory, and more confidence in reading it. Together with my clinical judgment, this helps me catch these shifts before they become clinically obvious, gauge response to treatment over time, and decide whether an adjustment is needed.
How Digital Cognitive Assessment Reduced My Diagnostic Uncertainty
Digital assessment tools have markedly reduced diagnostic uncertainty in my practice and the group practices I manage. Standardized delivery, automated scoring, and ongoing tracking of cognitive performance let me monitor treatment progress and outcomes more effectively. Since incorporating Creyos, I can detect subtle cognitive changes earlier, better distinguish between psychiatric and neurodegenerative conditions, engage more meaningfully with patients, and determine when neurology referrals are appropriate – all of which allows my patients to receive the care they need more quickly.
A 59-year-old patient with a history of MDD presented for an initial evaluation with depressive symptoms and memory problems, describing themselves as "so forgetful." When I asked them to explain, they said they were having trouble finding words in conversation, which made their job as a litigator difficult, but that they were "used to it" because they had experienced forgetfulness during prior depressive episodes. During the interview, I assumed their forgetfulness was mood-related and planned to reassess once their mood improved. However, Creyos testing suggested their memory problems were not exclusively mood-related. The data showed marked deficits in verbal memory despite otherwise intact cognition, which prompted a neurology referral. Ultimately, they were diagnosed with early Alzheimer's disease, allowing us to begin intervention and planning right away.
Making Cognitive Measurement Work in Real Psychiatric Practice
Several years ago, I was asked to open an outpatient practice for a large group of psychiatrists, building it from the ground up. Every policy, every protocol, every provider, and even every paperclip was my responsibility to write, create, hire, and source. The task was burdensome, but also exciting: I determined the workflow our providers would follow, which meant I was free to add or subtract elements as I saw fit. I had the unique opportunity to write digital cognitive assessment tools into the practice from the start. After extensive research, I selected Creyos, a scientifically validated cognitive assessment platform.
Buy-in as a Precondition for Sustainability
Of course, moving from idea to implementation is rarely smooth, and staff, providers, and patients all initially resisted the change to a familiar workflow. I quickly grasped how important buy-in from all three groups was to making the change stick. It wasn't enough to tell them Creyos was a fantastic addition. I had to show them the tangible, measurable advantages it provides.
I started with the providers, explaining how it would quantify symptom severity and let them track patient progress and response to treatment over time. When they learned it would inform their treatment decisions and support an evidence-based approach to care, their skepticism began to fade, and they decided to give it a try. Far from being intrusive or disruptive, these tools quickly proved invaluable, providing foundational support for assessment, diagnosis, and treatment planning. Once Creyos was part of the workflow, we gained insight into our patients' cognitive abilities that observation and self-report alone couldn't provide.
Adjusting workflows meant new steps for administrative staff as well, but I assured them it would soon become second nature and prove its worth through improved patient care – something everyone on the team wanted.
Last, we faced the challenge of convincing our patients that this tool was not optional, but a necessary part of their treatment plan. Introducing it required us to explain its purpose, benefits, and how it would directly improve their care. Many patients were initially skeptical. We addressed their concerns by taking the time to explain the science behind the assessments, and how the information would help us catch cognitive impairment earlier, tailor treatment plans, and help them feel better faster. Explaining why and how the tool mattered was critical to overcoming resistance at every level, and it helped us support our patients in promising new ways.
Integrating Creyos didn't require revamping workflows; instead, we identified points where the assessments fit naturally. We found that timing and flexibility in administering them not only minimized disruption but helped streamline diagnosis and treatment planning. Because the tool can be administered in the office or at home, you have some latitude in how much the in-office workflow needs to change. Digital tools can fit into the traditional workflow in many places, and finding the best fit for yours may take some trial and error.
At our clinic, we ask patients to complete their digital assessments one of two ways:
- In person at the office, right before or right after their appointment. This requires setting aside extra time, a quiet space, and a tablet.
- At home, right before leaving for or right after returning from their appointment. This requires a cell phone or desktop computer.
It is important to remember that any data, from any source, is only useful if we know how to read it, interpret it, and apply it. Creyos assessments are designed to capture a large amount of complex cognitive data quickly, score it, and present it in easy-to-interpret reports. Nevertheless, providers in our practice were trained to read these reports and navigate the platform during an easy-to-schedule online session with Creyos account executives.
From Gut Feel to Grounded Care: A Practice Transformed
When I first began using digital cognitive assessments, I was skeptical. Psychiatric assessment is perhaps the only type of medical assessment that relies almost exclusively on the patient interview. This doctor-patient interaction is essential, and it is the reason most of us entered this field in the first place – the humanness of psychiatry. I worried that this kind of technology would disrupt that relationship and distance me from my patients.
But it has done the opposite. The structured, objective data has helped me explain to patients why they are experiencing certain cognitive issues, and whether those changes are likely related to a psychiatric condition. This clarity reduced the uncertainty that once lingered between sessions, replacing it with a mutual understanding of their situation and a more focused treatment plan.
Incorporating digital cognitive tools into the traditional psychiatric workflow has transformed the way I support patients. These tools give me objective insight into cognitive performance, supporting more precise and personalized treatment plans. By blending technology with face-to-face care, I can track progress between sessions, intervene earlier when needed, and build a data-informed, collaborative approach to decision-making that empowers my patients to be active participants in their psychiatric care.


Written by Dr. Rebecca Reyes, Psychiatrist
Dr. Rebecca Reyes is a psychiatrist and leader in behavioral healthcare with dual degrees in medicine and law. She has held leadership roles across inpatient and outpatient settings, directed military/PTSD and substance abuse treatment programs, and served as both principal and sub-investigator in several phase 3 neuropsychiatry clinical trials. She is committed to evidence-based care, collaborative leadership, and advancing patient outcomes across diverse healthcare environments.