How Claremedica Made Cognitive Decline Visible Before It Became a Crisis

of organization-wide cognitive screening with traditional tools. Cognitive decline was affecting care everywhere, and they knew their approach wasn't capturing it.
clinical adoption of Creyos on day one, the highest across 10 go-lives in their disease detection program. Clinicians continue to champion the rollout.
of patients identified in the early and mild stages of cognitive impairment, early enough for proactive care planning and meaningful family preparation.
"Creyos hasn't just changed things for our patients and their caregivers.
It has changed the way our primary care providers think about what is possible when it comes to managing cognitive decline, and that is how you achieve better outcomes."
High-touch primary care built around early detection
Claremedica is a value-based primary care organization serving a culturally and linguistically diverse senior population across more than 35 sites in Florida. The high-touch care model means patients are seen 7 to 10 times annually, often by the same care team for years.
Their care model is built for prevention, not just response, and that logic shapes how they frame their main competitors. As Benjamin Todd, SVP of Strategy and Analytics, puts it, they see those competitors as systemic forces: a stale U.S. health care system, a chronic disease epidemic, and barriers to access.
Cognitive decline touched all 3 forces: a chronic condition slipping through an outdated screening approach, imperceptibly creating barriers for patients who were forgetting medications, missing appointments, and ending up in the hospital, without a system that equipped clinicians to connect these outcomes back to cognition.
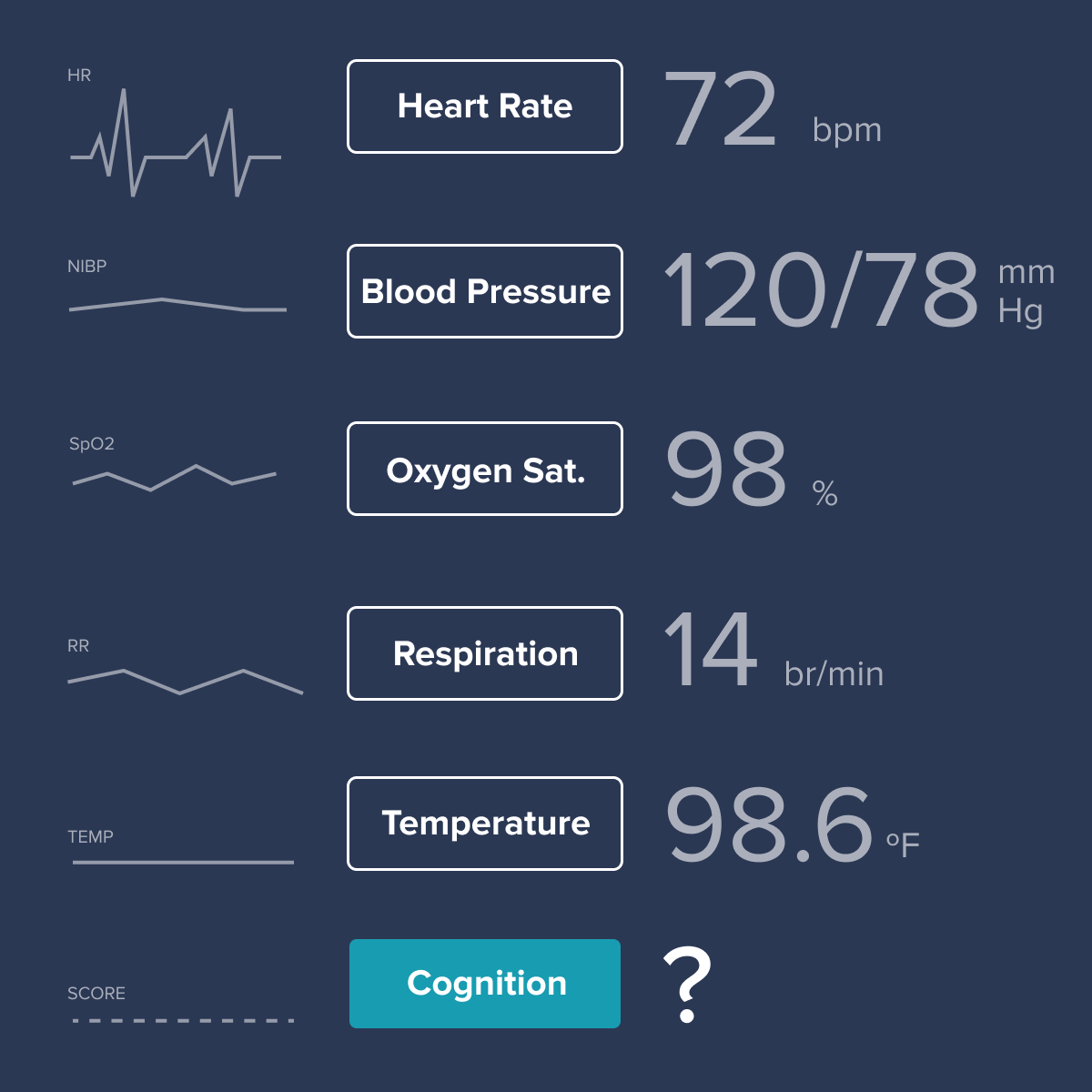
“In medicine, we're trained to look at vital signs: temperature, blood pressure, heart rate. But not cognition, which changes just as subtly over time. What would happen if we could?”
Adoption across 35+ sites without resistance
Before rollout, Claremedica invested in organizational alignment. They brought in Prof. Adrian Owen, PhD, Neuroscientist and Chief Scientific Officer at Creyos, to present to every staff member across the organization on the opportunity ahead.
"We shut down operations across the entire organization to tune in for an hour," Dr. Gheewala shares. "We have never had a leader come in and convey the clinical outcomes improvement that we were about to walk into. A year into this, we're happy to say they were right." The result was buy-in at every level, from primary care physicians to front desk staff to coding and analytics teams.
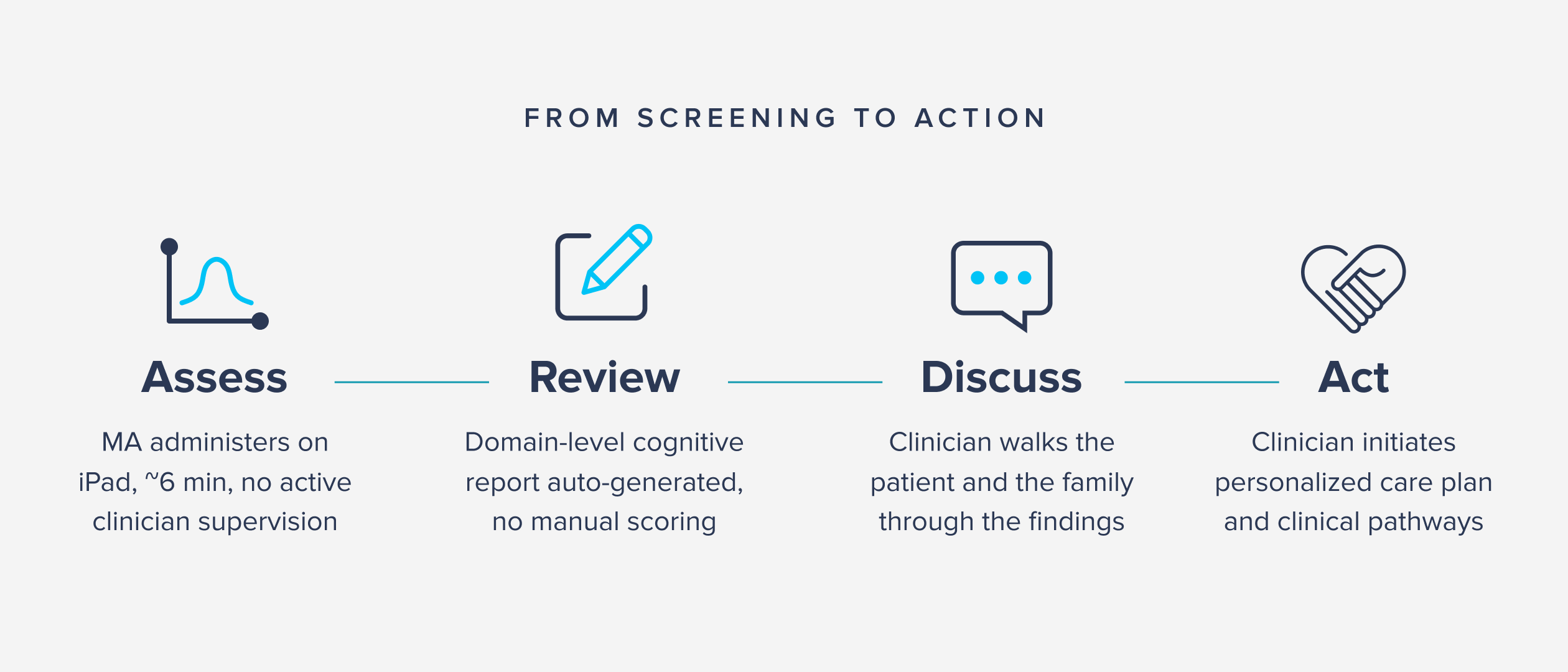
As implementation progressed, Claremedica built clinical pathways that connected Creyos results to concrete actions, including:
- medication review;
- chronic disease management;
- depression and mood screening; and
- social engagement.
Each Creyos assessment generated a report clinicians could open and review with the patient still in the room, and wide-spread adoption quickly followed. Clinicians "admitted that they had never seen anything like this that was so easy to implement and also easy to discuss with the patient," Dr. Gheewala shares.
Change is rarely smooth in established clinical workflows, especially among clinicians trained to be cautious about new tools. Dr. Gheewala describes Creyos as an outlier from day one, with clinicians continuing to express enthusiasm about the tool, the implementation, and the patient conversations it enables. As Benjamin puts it, "Adoption was so immediate that on even the busiest days, the only bottleneck was iPad battery life."
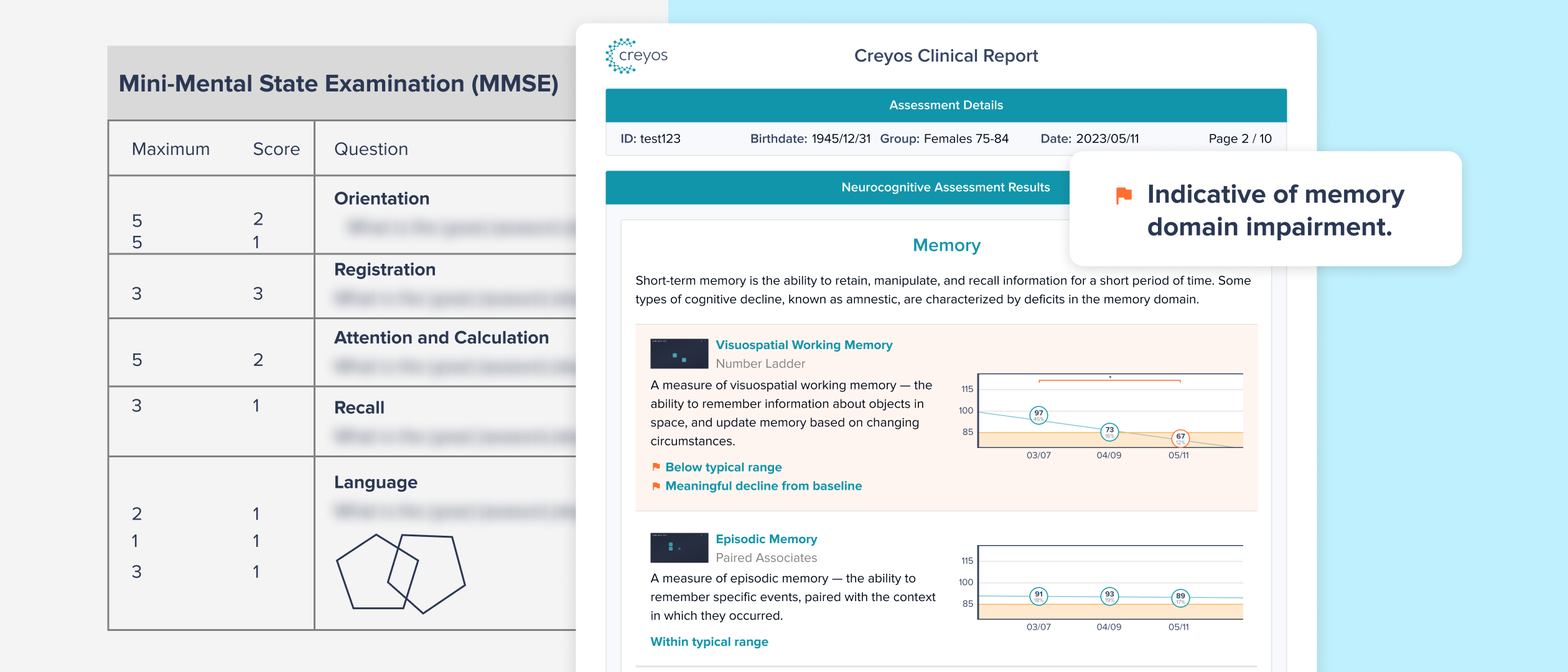
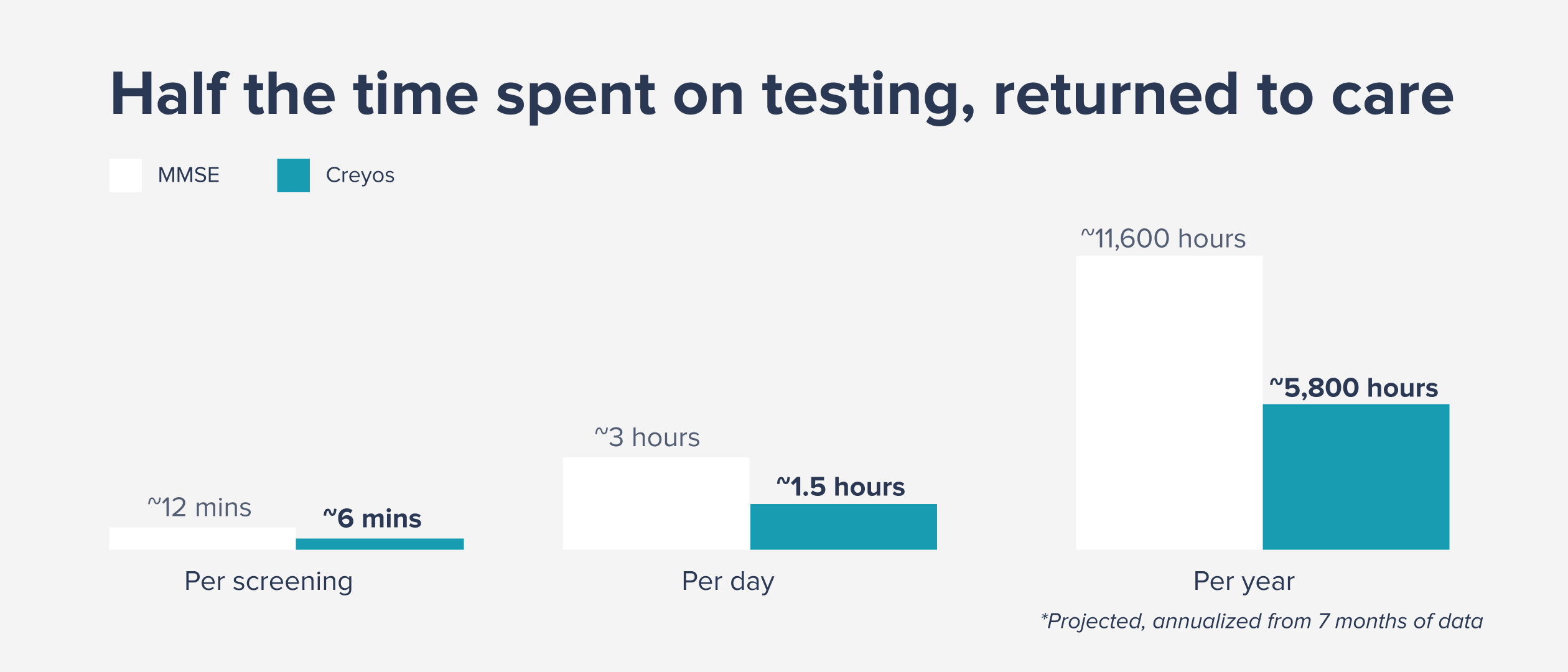
The operational impact was equally significant. Average screening time dropped from roughly 12 minutes with the MMSE to 6 minutes with Creyos. That baseline reflected Claremedica's commitment to administering the MMSE by the book, with some PCPs taking 15 to 20 minutes themselves to ensure thoroughness.
Across a typical clinician caseload of 15 to 16 patients per day, that translates to roughly 90 minutes returned to each clinician daily. In a value-based care model, that time goes directly back to patient-facing care: discussing results, coordinating next steps, and having the kinds of conversations that build trust between a clinician and the patients and families in the practice.
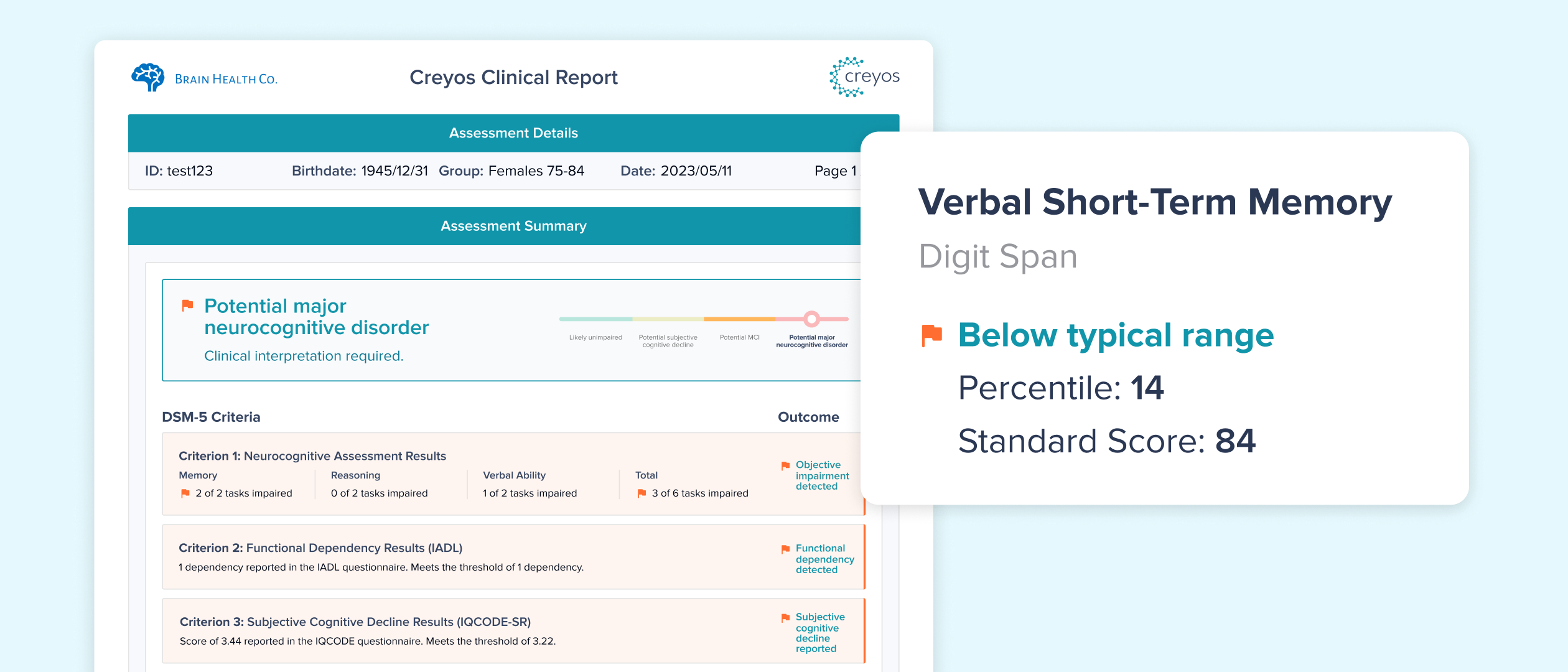
What made the difference was not just detection, but the quality of the clinical information. Each Creyos assessment captures domain-level data that Claremedica's providers can trend across visits. This objective, deeper insight, Dr. Gheewala says, is what enables clinicians to show families what is happening and what to do next.
That specificity has shifted how Claremedica clinicians approach cognitive health. Their front-line physicians now treat cognition the way any other vital measure would be trended. Several clinicians have begun requesting additional assessments on their own, based on what is being observed clinically. "People are still beaming every time they talk about it," Benjamin says.