
The Montreal Cognitive Assessment (MoCA) is a 30-point cognitive screening test that takes approximately 10 minutes to complete and is used to detect signs of mild cognitive impairment (MCI). It is a screening tool rather than a diagnostic test: a low score signals the need for further evaluation rather than confirming dementia.
Despite the popularity of the MoCA test among 63.8% of medical experts, up to 40% of primary care providers (PCPs) report that they don't feel confident making a dementia diagnosis. When it comes to dementia care, it's early detection that creates the opportunity to improve patient outcomes.
Screening tools like the MoCA aren't detailed enough for PCPs to confidently diagnose dementia, and in-depth neuropsychological exams can take over a month to schedule. This gap in dementia detection shows there's a need for evidence-based assessments that are sensitive enough to catch earlier signs of Mild Cognitive Impairment (MCI), quicker to deliver accurate results to support diagnosis, and while there is still time to slow cognitive decline and plan for care.
In this article, we discuss the strengths and limitations of the MoCA test and how it compares to newer computerized cognitive assessment tools. We show how computerized testing procedures have the potential to fill the gap in detecting mild cognitive impairment, leading to more effective brain health treatments and better dementia care for patients.
Article Highlights
The MoCA is a widely used screening test, not a diagnostic tool, and its cutoffs are contested.
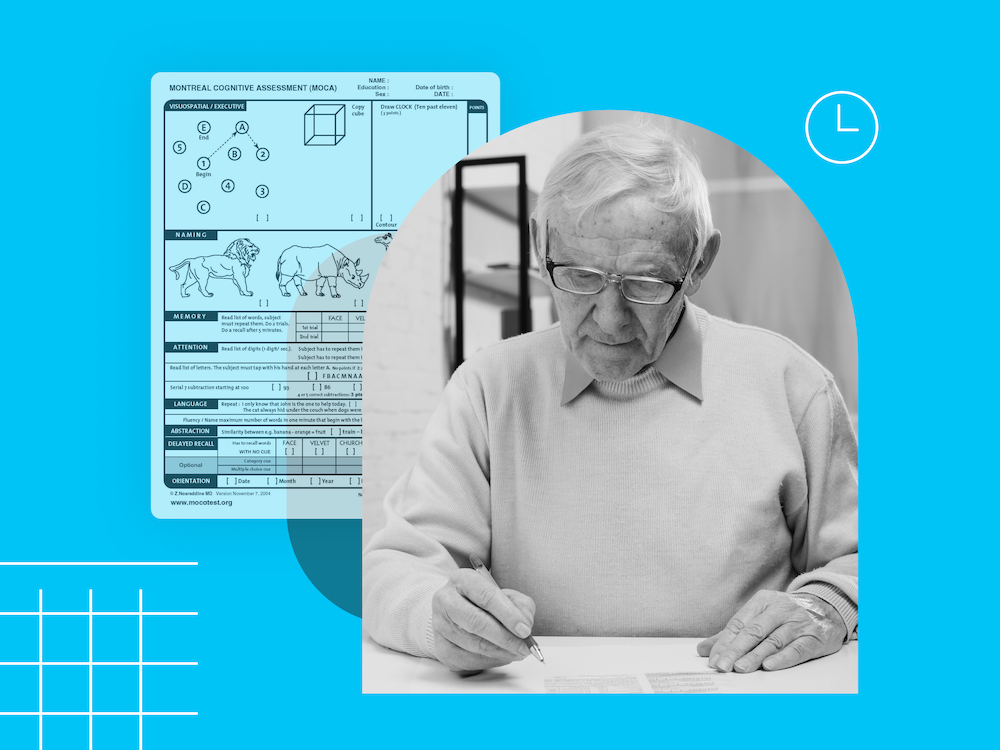
- The MoCA is an 11-exercise, 30-point test that takes approximately 10 minutes, with 26 or higher considered normal cognition.
- The standard MCI cutoff of 26 is sometimes questioned, with different studies recommending different cutoffs.
- Administering and scoring the MoCA requires certification training.
- Up to 40% of primary care providers report they do not feel confident making a dementia diagnosis.
What is the MoCA test?
The Montreal Cognitive Assessment is an eleven exercise cognitive test that takes approximately 10 minutes to complete. The MoCA was initially created in 2005 to improve upon the Mini-Mental State Examination (MMSE), which often fails to identify individuals with MCI.
Like all screening tests, the MoCA is considered a form of preventive care, as it is designed to detect mild cognitive impairment if conducted as part of a regular healthcare checkup. However, specialized testing via a neuropsychological exam is sometimes required to gather more detail or determine the source of a patient's cognitive difficulties: Alzheimer's disease, Parkinson's disease, vascular dementia, Lewy body dementia, or something else. Furthermore, the MoCA may have difficulty detecting milder declines in cognition before there is obvious subjective concern.
When is the MoCA test used?
The MoCA test can be implemented as soon as a patient expresses that they're experiencing symptoms of cognitive dysfunction. If required, a primary care provider can then refer the patient to a neurologist for further testing. The neurologist might administer the MoCA as well, using it as a screener to test cognitive function before a neurological exam or other assessments. When cognitive deficits are confirmed and potential causes identified, a cognitive care plan can be created to enhance their quality of life, monitor treatment efficacy, detect changes to symptoms, and support their cognitive maintenance.
How to score the MoCA test
The patient's condition is assessed by calculating a total score across 11 exercises, with a maximum score of 30. According to the MoCA website, if a patient has a total score of 26 or higher, their cognitive health is considered normal, with normal cognition. Scores of 18 to 25 can indicate mild cognitive impairment, while scores of 10 to 17 can suggest moderate impairment. A score of less than 10 indicates severe impairment. Administering the MoCA and scoring a patient's answers requires certification training.
What are the strengths and limitations of the MoCA test?
Once a primary care provider knows the MoCA's pros and cons, they can compare it with other assessments and make an informed decision on what's best for their practice and patients.
| Strengths | Limitations |
|---|---|
| Ease of use: The MoCA only takes 10 minutes to administer and is available in pen-and-paper or computerized formats. | Uncertain cutoffs: The standard cutoff for MCI is a total score of less than 26, but this is sometimes questioned, with different studies recommending different cutoffs. Many patients are also considered borderline if they are close to the cutoff, which leaves healthcare professionals without clear answers. |
| High sensitivity for severe deficits: It has a high chance of accurately screening a patient for cognitive dysfunction once they start displaying clear symptoms. | Inaccurate for certain populations: A study found that MoCA tests administered in diverse, urban communities resulted in a significant number of false positives for cognitive impairment. Additionally, in old-age psychiatric settings, specificity may not be as high as in lab-based estimates. |
| Availability: The MoCA test is available in nearly 100 different languages and has variations for people with blindness or impaired hearing. | Impacted by mental health conditions: Certain mental health conditions, like depression, which is often comorbid with dementia, can impair cognitive function, meaning that the MoCA alone may not be able to identify the cause of symptoms. |
| Low cost: Unlike the MMSE, the MoCA is usually free for clinical use, though training and certification are considered mandatory. | Inappropriate for long-term monitoring: The MoCA's simple exercises can be prepared for or even memorized. Though there are multiple variations available, practice effects can still make interpretation difficult when doing repeat testing. |
Alternatives to the MoCA for dementia screening and assessment
The Creyos platform is available to expedite the screening and diagnostic process, deliver accurate results, and support patient care and quality of life. Each tool is more detailed than traditional screening tools like the MoCA and quicker than full neuropsychological exams, while also being available through the convenience of an online, telemedicine-friendly platform.
Screen for impairment
The two-task cognitive screener is comparable to the MoCA, but takes approximately five minutes to complete. The Creyos dementia screening test can detect subtle signs of cognitive impairment, and doesn't require training to administer or interpret. The screening results will indicate whether further testing is recommended to assist in the diagnosis of dementia or MCI.
Assess cognitive skills
If further testing is required, Creyos includes an assessment that provides detailed information about cognition in 20 minutes or less, which may assist with an accurate diagnosis. The assessment is a highly sensitive and scientifically validated six-task protocol. Once complete, it generates an easy-to-interpret report based on DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) criteria for mild and major neurocognitive disorders. This allows healthcare professionals to quickly gain much of the information comparable to a neuropsychological exam, informing diagnosis, monitoring, and treatment plans.
Create a care plan
Once a diagnosis is reached, Creyos comes with a built-in cognitive care plan. The care plan is based on guidelines by the Alzheimer's Association, and allows PCPs to provide support for caregivers and enhance patient quality of life. After a care plan is in place, cognitive assessment can be repeated to track treatment effectiveness and monitor patient symptoms over time, so PCPs can collect longitudinal data and make objective clinical decisions about next steps.
How Creyos compares to the MoCA
While the MoCA can be a useful tool to screen for cognitive impairment in patients, it takes more work on a PCP's part to use it effectively and accurately.
To do so, healthcare professionals need to:
- Be trained and certified to administer, score, and interpret MoCA test results
- Account for potential mental health conditions in a patient
- Refer patients (if MCI is detected) for a prolonged neuropsychological examination
And even if a PCP follows these steps, there's always a chance that the results of the MoCA may be inaccurate due to factors like education or early symptoms that go undetected.
While the MoCA is used in many practices offering cognitive screening, healthcare professionals may want to consider additional options, like the Creyos cognitive assessments. These computerized neuropsychological assessments offer additional insights that aren't offered by the MoCA and MMSE, while also being patient-friendly and efficient for clinicians. With the need for fewer referrals, this can free up providers' time and lead to greater patient retention.
In one study comparing the MoCA and Creyos tests, borderline patients, those close to the MoCA cutoff, could be more confidently classified as impaired or unimpaired using a short set of Creyos tasks.
The Creyos assessments bridge the gap between an initial screening test (like the MoCA) and a neuropsychological exam, allowing providers to easily incorporate them into a more thorough testing process and improve dementia care. Additionally, the results are easy to interpret, don't require special training, and are instantly tabulated and compared to a diverse 85,000+ person normative database for demographic-specific results.

When should you use a computerized cognitive assessment?
The Creyos Health platform is flexible enough to assess cognitive function in a wide variety of patients and use cases. Unlike the MoCA, the 20-minute Creyos assessment can be used to gain detailed information about multiple cognitive domains, compare the patient to age-matched norms, and includes mental health questionnaires, allowing PCPs to consider a patient's mental health conditions when assessing cognitive deficits.
Compared to traditional cognitive tests like the MoCA or MMSE, the computerized cognitive testing at Creyos is able to provide healthcare professionals with more detailed insight into a patient's cognition, while giving them the benefit of being tested at their own convenience.
Additional benefits of Creyos Health
- Scientifically robust and clinically sound tools with objective results
- Gamified, approachable user experience for better patient engagement
- Built from the ground up to support remote administration for greater accessibility
- Non-memorizable and ideal for retesting
- Electronic medical record (EMR) integrations
Bridging the cognitive care gap in neurology
While the MoCA is an accurate test when used as an initial screening tool for existing mild cognitive impairment, its disadvantages make it less appropriate as a diagnostic aid for MCI and dementia.
Instead of relying solely on the MoCA, consider bridging the dementia detection gap with highly sensitive computerized assessments. With digitized testing, primary care providers can increase the chances for early detection of MCI and dementia, expedite diagnosis, and enhance their patients' quality of life by getting them the right care before the disease progresses.


Reviewed by Mike Battista, Director of Science & Research at Creyos
Mike Battista specializes in brain health, cognition, and neuropsychological testing. He received his PhD in personality and measurement psychology at Western University in 2010 and has been doing fun and useful stuff in the intersection between science and technology ever since.