
When it comes to treating cognitive impairment, early intervention is essential for delaying the onset of Alzheimer’s disease and other forms of dementia. Not only does this improve patient and caregiver quality of life, but it also significantly reduces the cost of care.
While the Montreal Cognitive Assessment (MoCA) test is a commonly used dementia screening tool, it doesn’t meet all of the Alzheimer’s Association (AA) recommendations for effective dementia screening and may not be accurate enough to use alone. In this article, we will explore the way new AA guidelines apply to the MoCA and discuss the advantages of digital alternatives for cognitive screens.
Key Takeaways: Assessing Cognitive Impairment
|
The Diagnostic Accuracy of the Montreal Cognitive Assessment
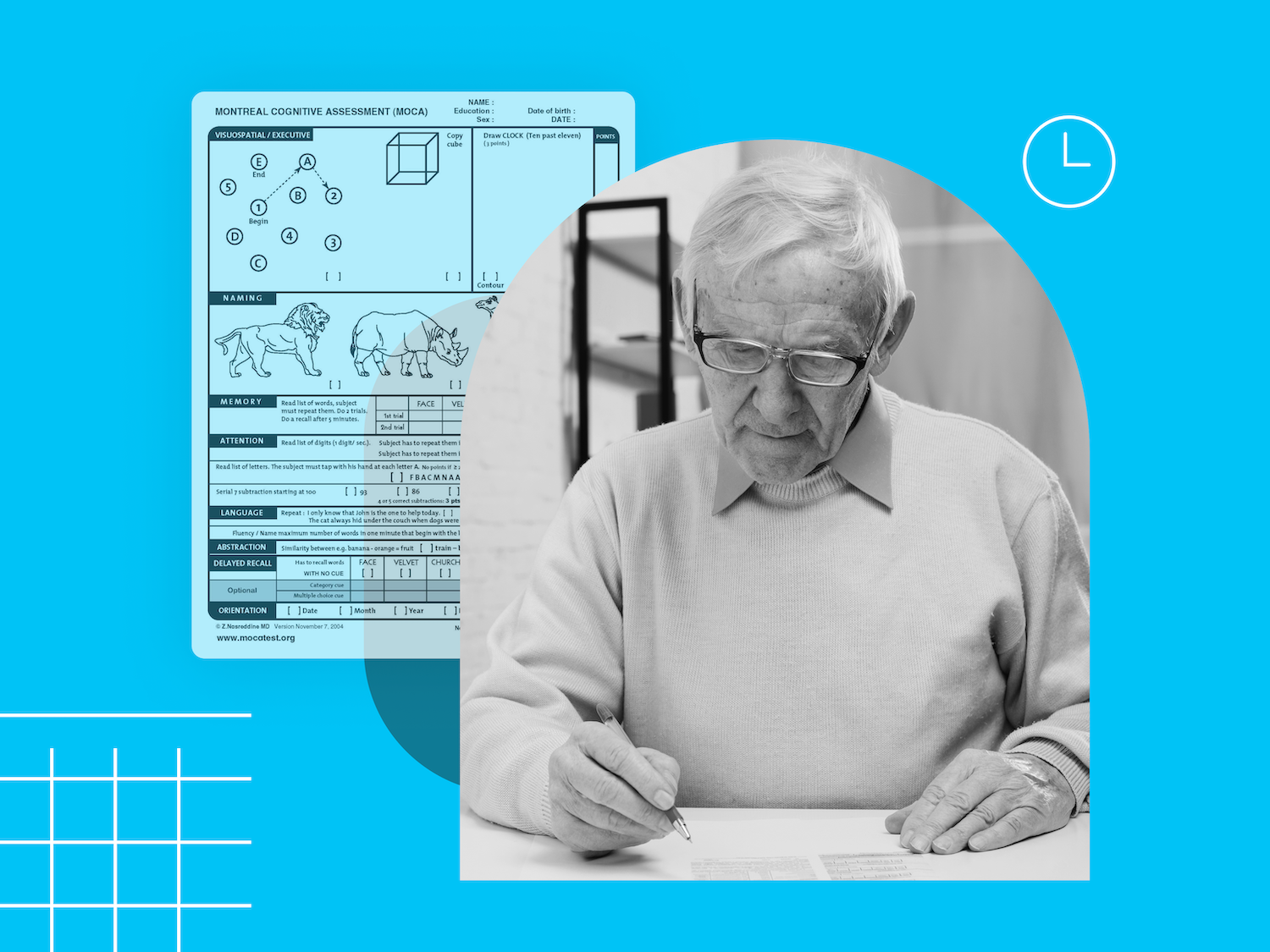
The Montreal Cognitive Assessment was developed by Dr. Ziad Nasreddine in 1995 for the detection of mild cognitive impairment (MCI) in clinical practice. Since then, it has become a popular cognitive screening tool for healthcare professionals in hospitals, neurology practices, and primary care settings.
Currently available in over 30 languages, the MoCA can be completed in under 10 minutes. However, it does require a trained professional to accurately interpret results. While it cannot provide a formal diagnosis of MCI or dementia, it is often used as an initial screening tool to detect cognitive deficits.
The MoCA is a 30-point test, where a score of 26 or higher is considered normal. A high score requires high functioning in multiple cognitive domains that may be impaired in dementia patients, including the following:
- Memory
- Executive functioning
- Attention
- Language
- Visuospatial
- Orientation
While the MoCA has been used to accurately flag signs of advanced cognitive dysfunction, it requires additional follow-up testing after use to determine if dementia is present and what type of dementia a patient may be exhibiting signs of.
How accurate is the MoCA?
The Montreal Cognitive Assessment can be effective for identifying signs of pronounced cognitive impairment, but it lacks specificity and may not pick up on earlier, subtler signs of MCI. A Cochrane review found that while the MoCA was able to correctly identify over 94% of people with dementia, it also recorded a high number of false positives. In fact, over 40% of people without dementia scored under 26 points and would have been falsely flagged for dementia if their provider had used the MoCA alone.
These limitations may be related to the MoCA’s susceptibility to:
- Ethnocultural, linguistic, and education-based biases: In one study based in an urban setting, the current MoCA cut points were found to be inadequate in a culturally diverse population, even when including the Spanish-language MoCA.
- Inability to account for comorbid mental health conditions: Conditions like depression, which are frequently comorbid with dementia, can affect or impair cognitive function and performance. Tests like the MoCA cannot distinguish if impairment is due to dementia or a comorbidity.
- Impaired vision and/or hearing: Results of a cognitive function test may be inaccurate or skewed if visual or auditory disabilities challenge the patient’s capacity to execute the test.
2026 Alzheimer's Association Recommendations: Does the Montreal Cognitive Assessment Pass the Test?
When we compare the MoCA to the Alzheimer’s Association’s recommendations, the assessment meets only 3 out of 5 of the organization's criteria for an effective cognitive screening tool.
While the MoCA is commonly used in primary care settings, is correctly used as a screener for further testing, and is superior to some other options, the test does not meet some of the other requirements mentioned by the Alzheimer’s Association. For instance, the test:
- Is not able to be be administered in under 5 minutes
- Is not free of educational, language, and/or cultural bias
As with any brief initial screener for cognitive decline, the Montreal Cognitive Assessment does not have the capacity to accurately diagnose dementia on its own. If a patient fails a cognitive function test, this may be an indication that further evaluation or a specialist referral is warranted.
Using the MoCA vs. Digital Cognitive Testing in Clinical Practice
On its own, the MoCA may not have the diagnostic capabilities or detail to give a full look at cognitive function. Initial assessments are a key step in clinical practice for flagging symptoms of cognitive dysfunction, allowing providers to confidently refer patients for further neurocognitive testing.
In an overtaxed system, avoiding unnecessary referrals saves time and money for patients and providers. That’s where digital screening testing tools come in. Combining the MoCA with digital cognitive screens is a powerful way to gather the data providers need to deliver quality care.
Advantages of Digital Cognitive Screening
Compared to traditional pen-and-paper screens like the MoCA, digital cognitive assessments carry several advantages:
- Virtual or in-clinic administration: Enabling enhanced accessibility standards so that patients residing in remote locations or with mobility concerns can still receive high-quality care.
- Reduced cultural, linguistic, and educational bias: Some digital, nonverbal, visual assessments rely less on language and education level, making results more comparable across diverse populations.
- Faster administration and scoring: Tests are automatically scored, and reports are directly integrated into EHRs, leaving more time for providers to focus on delivering personalized medical care.
- Higher retesting value: Monitoring objective changes to cognitive function can more precisely detect decline from a personal baseline or track the effectiveness of treatment longitudinally with test items that are randomly generated at each administration.
Research suggests that evidence of dementia-related cognitive dysfunction can be detected up to 9 years in advance. Accurate digital tools can catch subtle symptoms that tools like the MoCA test may not, while also minimizing false positives, allowing for the earliest possible intervention for the right patients.
Creyos: A Digital Tool for the Assessment of Mild to Severe Cognitive Impairment
The Creyos Dementia Assessment is a scientifically validated, digital testing battery designed to support early dementia detection and ongoing monitoring in clinical practice. It simplifies screening practices while also providing objective, detailed insight into patient cognition.
Our dementia protocol includes three key components:
Online Cognitive Tasks
Brief, gamified online cognitive tasks measure cognitive domains that have been shown to be associated with dementia and affected by mild cognitive impairment. The two-task screener can be completed in under five minutes either remotely or in person and is scored instantly to determine if further testing is required.
Signs of cognitive impairment can be initially assessed using a two-task screener. The screener portion of the assessment is most similar to the MoCA and can be administered on its own or as part of a more comprehensive assessment that includes four additional cognitive tasks to provide more detailed information about cognition. These tasks assess:
- Episodic memory
- Visuospatial working memory
- Attention
- Verbal short-term memory
- Mental rotation
- Response inhibition
By analyzing performance across multiple cognitive domains, the assessment can help clinicians distinguish normal aging patterns from MCI or dementia. This improves its diagnostic assistance compared to brief screening tools like the MoCA alone.
Behavioral and Mental Health Questionnaires
In addition to objective cognitive tasks, the Creyos assessment includes standardized questionnaires that capture subjective patient information. These data help clinicians put results in context or identify comorbidities that may be influencing cognitive function.
Included questionnaires assess the following:
- Subjective cognitive complaints (IQCODE)
- Instrumental activities of daily living (IADL)
- Depression symptoms (PHQ-9)
- Anxiety symptoms (GAD-7)
Care Planning and Ongoing Monitoring Tools
Creyos extends beyond assessment with built-in tools that can use results as part of clear, actionable, and personalized care plans.
Key care planning features include the following:
- Pre-packaged cognitive care plans tailored to individual profiles
- Task-level retesting for monitoring progression or treatment response
- Automated reports that integrate directly into EHR systems
This streamlined approach reduces administrative burden while enabling ongoing tracking of cognitive impairment over time. Creyos also supports documentation needs related to the CMS-HCC V28 Medicare Advantage risk adjustment system, allowing both your patients and practice to thrive.
Creyos and Alzheimer’s Association Recommendations
When it comes to recommendations from the Alzheimer’s Association, the Creyos Dementia Protocol is aligned in 5 key ways:
- It includes a two-test initial screener that can be completed in under five minutes
- It is scientifically-validated in clinical settings, and used in one of the world’s largest dementia trials
- It is equal to or superior to the MMSE in specificity for a full picture of cognitive health
- It is easy to administer by non-physicians and designed to reduce educational, language, and/or culture biases
- It includes both a screener and a detailed assessment to further support next steps or referral to a specialist
Backed by hundreds of studies and large-scale research trials, plus real-world use in neurology and primary care settings, Creyos delivers scalable testing with high accuracy for modern dementia care.
Managing Cognitive Decline in Global Aging Populations
As the number of people with dementia continues to rise worldwide, healthcare providers need practical ways to adapt and better support patients experiencing cognitive dysfunction. Cognitive screening is evolving, and the shift away from tools like the Montreal Cognitive Assessment toward more detailed digital screening and assessment tools is a positive step forward.
By normalizing and simplifying cognitive assessment, providers can stay ahead of dementia care—benefiting patients, families, and clinical teams alike.

 Reviewed by Mike Battista, Director of Science & Research at Creyos
Reviewed by Mike Battista, Director of Science & Research at Creyos
Mike Battista specializes in brain health, cognition, and neuropsychological testing. He received his PhD in personality and measurement psychology at Western University in 2010 and has been doing fun and useful stuff in the intersection between science and technology ever since.